TM is a neurological disorder caused by inflammation across both sides of one level or segment of the spinal cod. Myelitis means inflammation of the spinal cord and transverse describes the position of the inflammation. Inflammation can damage or destroy myelin. The damage causes nervous system scars that interrupt the communication between the nerves in the spinal cord and the rest of the body. Most clients recover from TM with minor or no residual issues, while others suffer permanent impairments. TM affects any gender, race, and age. Common symptoms include: localized lower back pain, sudden pain in legs, sensory loss, and bowel and bladder issues. The symptoms can develop over a few days or weeks. The most common therapy for TM includes keeping the body functioning, in hopes of a partial or complete recovery. Caregivers may be instructed to manually move a clients limbs to keep the muscles flexible and strong. If limb control is recovered, then other therapies may be started, like OT. This is where bingo can help!
Joe likes going to sporting events, especially hockey and basketball. I wanted to create a game to bring out his competitive side. I incorporated different types of sports with strengthening and stretching activities. My hope is that therapy would not be boring to Joe, but something that he looks forward to doing to get better. Joe has very little lower body strength. The exercises on the bingo board are designed to strengthen and stretch his legs in hopes of a faster recovery. A few items on the board are focused on the upper body. This is to give Joe a break, so that his legs do not get tired. In order to cover up a space on the board, Joe will have to successfully complete the exercise. Four successful exercise completions in a row equals a bingo! Joe has a close knit family. As a prize for completing a bingo card, I thought it would be a good idea for Joe's family to take him to a sporting event. This brings the family into helping Joe be successful in therapy.
The goals for Joe are as follows:
Those with TM are not the only clients, who can benefit from chair bingo. TM is very similar to Guillain Barre Syndrome. They both attack the nerves and a client can recover over time. Anyone who has a spinal cord injury in the thoracic vertebrae or lower may be able to benefit from this game. Chair bingo can always be graded up or down.
The goals for Joe are as follows:
-Joe will attempt to complete one card each
week.
-Joe will practice two of the exercises off
the “chair bingo” card every other day.
-Joe will increase leg strength from 2/5 to
3/5 in three weeks.
Description of the exercises. (All exercises are to be performed while sitting in a wheelchair, chair, or on a therapy mat.)

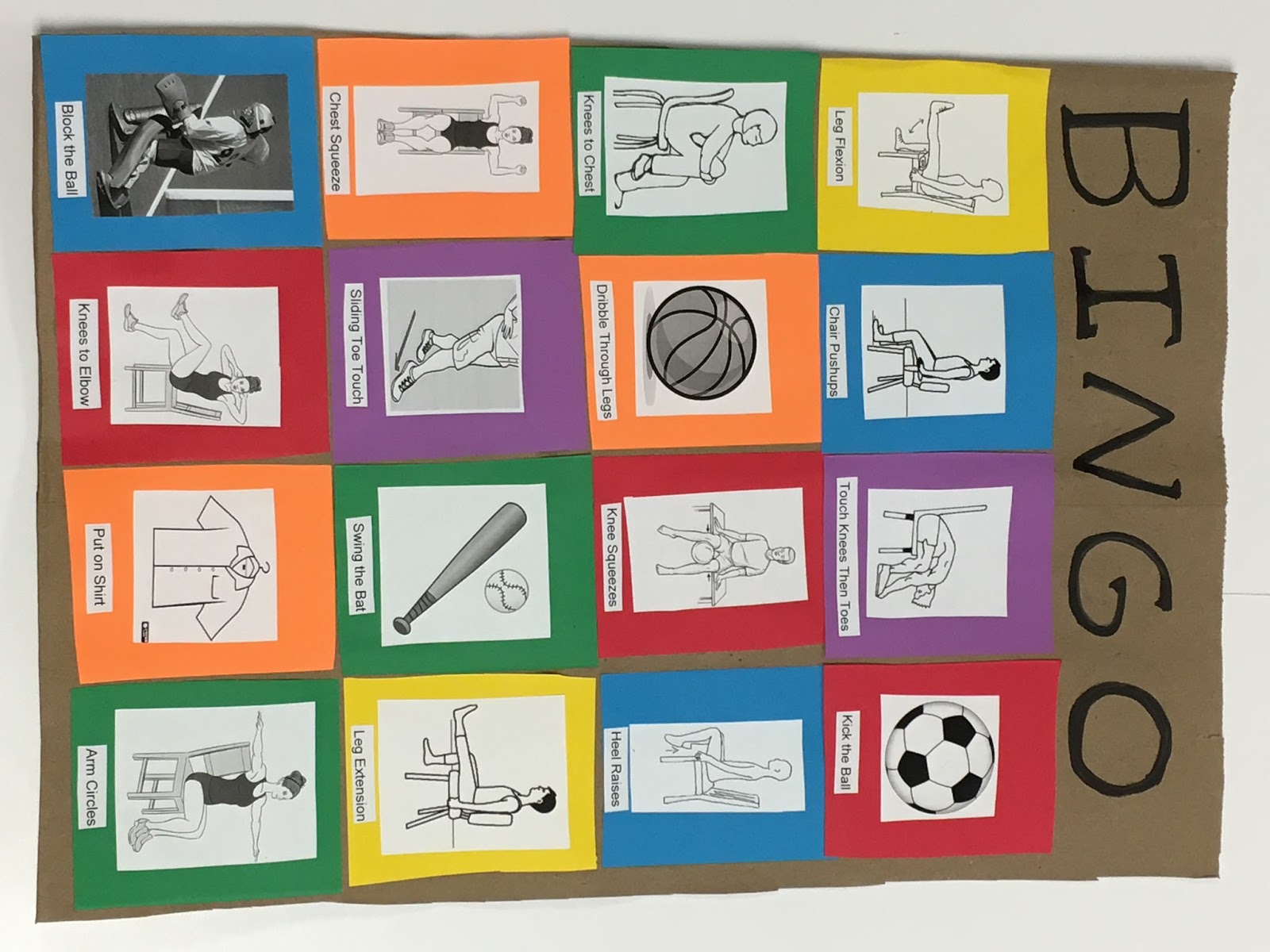
-Chair push ups-Client will place hands on arm rests, as close to shoulder as possible, and push up.
-Leg extension-Client will raise leg into extension
-Knees to chest-Client will bring knee to chest
-Leg Flexion-Place a rolled towel under knee. Client will move knee as far back as possible into flexion.
-Heel raises-Client will lift the heel up and down
-Knees to elbow-Client will bring elbow to knee while keeping chest firm.
-Chest squeeze-Client will hold arms at 90 degrees with elbows bent and push arms together.
-Arm circles-Client will hold arms perpendicular to the body and circle counter clockwise or clockwise.
-Block the ball-Client is the goalie. They will move legs side to side as one unit to keep ball from getting past them.
-Kick the ball-Client will kick the ball
-Swing the bat-Client will hold arms like swinging bat back an forth in a slow, controlled manner. (emphasis on extending arms during swinging motion)
-Put on a shirt-Client will put on and take off a shirt
-Knee squeezes-A ball will be placed between clients knees. Client will squeeze knees together.
-Sliding toe taps-Client will extend leg out and tap pointed toe
-Dibble through legs-Client will take a basket ball and dribble through legs.
-Touch knees then toes-Client will bend for hands to touch knees and stretch towards toes.





Hope everyone finds this helpful!!
